Breast Reconstruction Before & Afters
This category contains nudity. Please click OK to confirm you are at least 18 years of age and are not offended by such material.
![breast reconstruction Before & After Image]() Before
Before![breast reconstruction Before & After Image]() After
After![breast reconstruction Before & After Image]() Before
Before![breast reconstruction Before & After Image]() After
After![breast reconstruction Before & After Image]() Before
Before![breast reconstruction Before & After Image]() After
After![breast reconstruction Before & After Image]() Before
Before![breast reconstruction Before & After Image]() After
After![breast reconstruction Before & After Image]() Before
Before![breast reconstruction Before & After Image]() After
After![breast reconstruction Before & After Image]() Before
Before![breast reconstruction Before & After Image]() After
After![breast reconstruction Before & After Image]() Before
Before![breast reconstruction Before & After Image]() After
After![breast reconstruction Before & After Image]() Before
Before![breast reconstruction Before & After Image]() After
After![breast reconstruction Before & After Image]() Before
Before![breast reconstruction Before & After Image]() After
After![breast reconstruction Before & After Image]() Before
Before![breast reconstruction Before & After Image]() After
After![breast reconstruction Before & After Image]() Before
Before![breast reconstruction Before & After Image]() After
After![breast reconstruction Before & After Image]() Before
Before![breast reconstruction Before & After Image]() After
After![breast reconstruction Before & After Image]() Before
Before![breast reconstruction Before & After Image]() After
After![breast reconstruction Before & After Image]() Before
Before![breast reconstruction Before & After Image]() After
After
 Before
Before After
After Before
Before After
After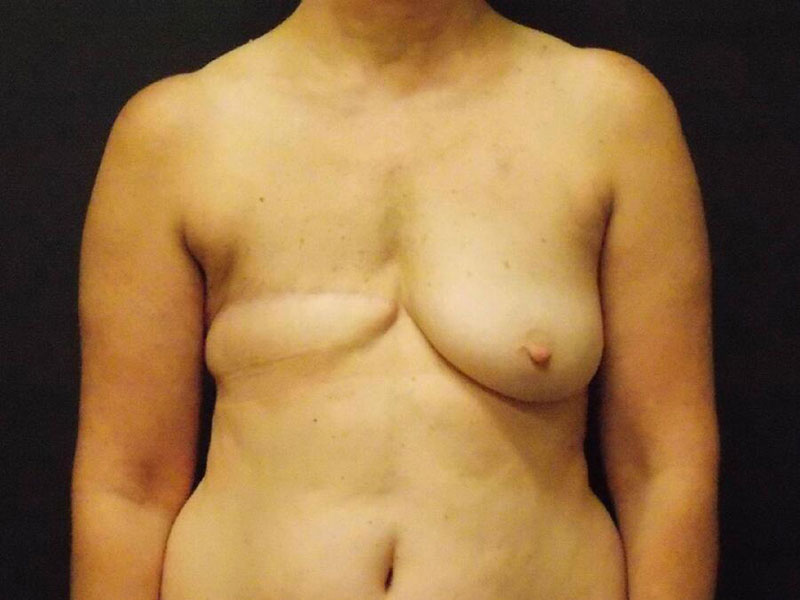 Before
Before After
After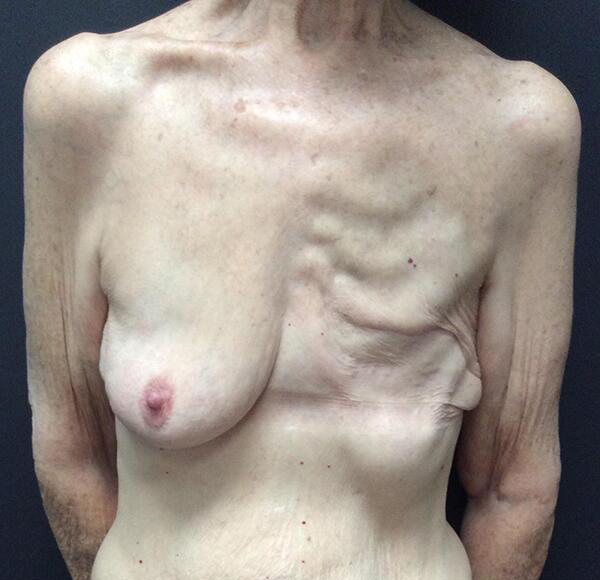 Before
Before After
After Before
Before After
After Before
Before After
After Before
Before After
After Before
Before After
After Before
Before After
After Before
Before After
After